On paper, a non-contrast head CT looks like one of the easiest things a radiology team will ever bill. One scan, one code, done. In practice, CPT code 70450 sits inside a three-code family where a single same-day decision running a second scan with contrast can flip a perfectly correct claim into a denied one.
This guide covers what the code actually describes, when to reach for it instead of its siblings, which modifiers belong on it, the bundling rule that trips up even experienced coders, and how reimbursement is built. The goal is fewer denials and cleaner claims, not a glossary.
What CPT Code 70450 Covers
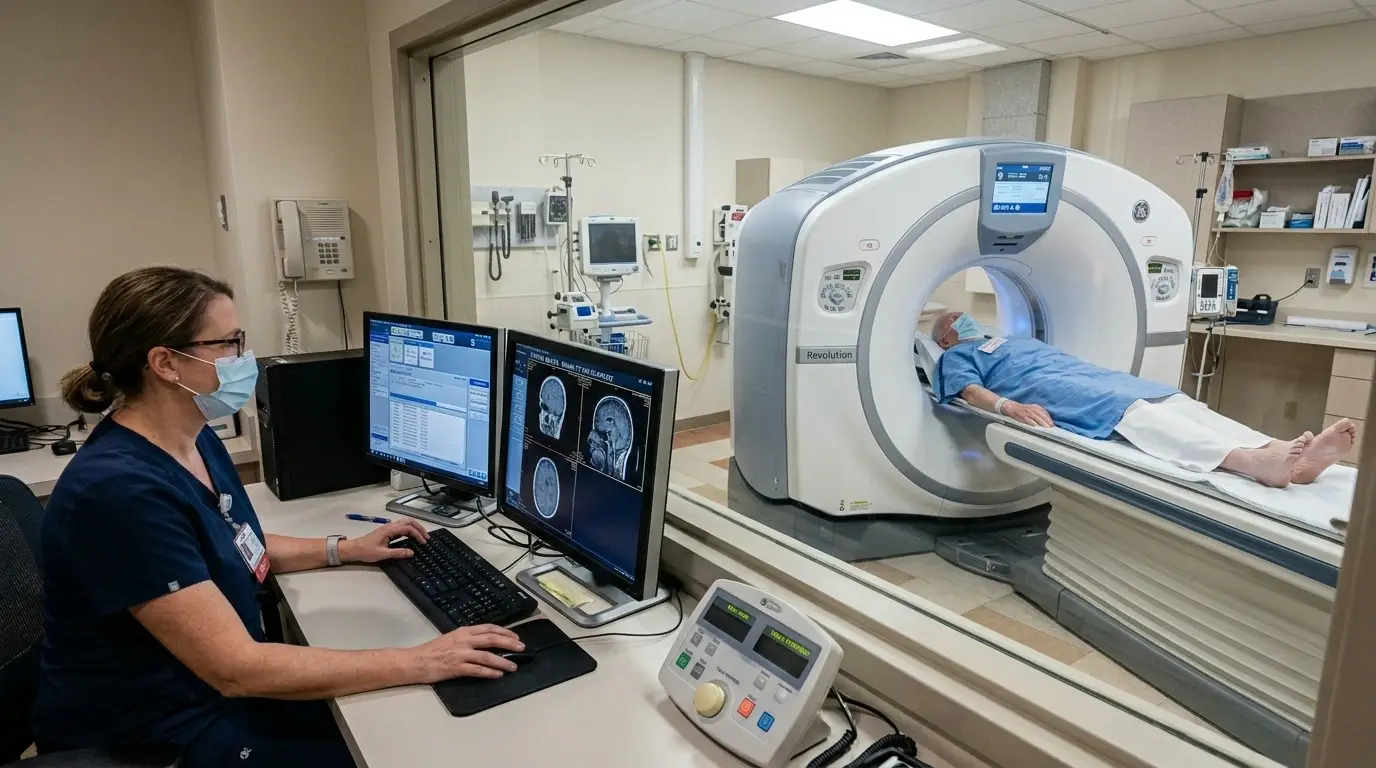
CPT code 70450 reports a diagnostic computed tomography (CT) scan of the head or brain performed without contrast material. It lives in the head-and-neck diagnostic radiology range. “Without contrast” means no iodinated dye was injected to highlight blood vessels or tissue; the study relies on standard X-ray attenuation alone, imaging from the vertex of the skull down to the foramen magnum.
Its job is to give clinicians a fast first look when something acute is suspected in the brain bleeding, trauma, stroke, or pressure changes. CT is high-volume work, too: according to UCSF research reported by NPR, about 93 million CT exams were performed in the United States in 2023, and head imaging is among the most common reasons patients enter the scanner.
Where 70450 Sits in the Head CT Code Family
The most common 70450 mistake starts with confusing it with the two codes next to it. The contrast status is the entire difference:
| Code | Descriptor | When it applies |
| 70450 | CT head/brain, without contrast | Standard non-contrast scan trauma, bleed, stroke |
| 70460 | CT head/brain, with contrast | Contrast study e.g., evaluating a suspected mass |
| 70470 | CT head/brain, without then with contrast | One combined study, both phases, same session |
Keep one more code in view: 70496 is CT angiography of the head, a separate study performed with contrast to evaluate vessels. It is not interchangeable with 70450, even when both are ordered together. Mislabeling these imaging studies is exactly the kind of error that drives radiology denials, which is why specialized radiology billing lean so heavily on coders who know the contrast-status distinctions cold.
When to Use CPT Code 70450
A non-contrast head CT is the preferred first-line image in several urgent situations: acute head trauma, sudden severe headache, suspected intracranial or subarachnoid hemorrhage, acute stroke or TIA, new-onset seizure in an unstable patient, and suspected hydrocephalus. In each case, contrast is not needed for that initial read fresh blood and gross structural changes show up clearly on a plain CT, and skipping contrast keeps the scan fast and avoids dye-related risk.
Acute Head Trauma in the ER
A patient arrives after a fall, confused and complaining of a headache. The emergency physician orders a head CT without contrast to rule out an intracranial bleed or skull fracture. The technologist performs the scan, and the service is reported with 70450 paired with the appropriate head-injury ICD-10 code.
Sudden Severe Headache
A patient describes the worst headache of their life with neurologic changes. The team suspects a subarachnoid hemorrhage and orders a non-contrast CT first, because acute blood is best seen without dye. Subarachnoid hemorrhage is uncommon roughly 10 to 14 cases per 100,000 people each year in the U.S., according to StatPearls (NCBI) but it is time-critical, which is why the plain CT comes first.
Suspected Acute Stroke
When a patient presents with sudden neurologic deficits, a non-contrast head CT is the standard tool to separate a hemorrhagic stroke from an ischemic one before any treatment begins. That single distinction changes the entire care path, and it is made on a 70450 study.
Technical, Professional, and Global Billing
Like most imaging codes, 70450 can be split into two parts: the technical work of running the scanner and the professional work of interpreting the images. How you bill depends on who did what.
Global Billing
When one entity both owns the equipment and reads the study, report 70450 with no component modifier. The single code covers the whole service.
Modifier TC
Append modifier TC when your facility performed the scan but a separate provider interpreted it. TC bills only for the equipment, staff, and supplies.
Modifier 26
A radiologist who interprets a scan performed somewhere else reports 70450 with modifier 26 for the read alone. Worth noting for imaging centers: a diagnostic non-contrast head CT requires only general physician supervision, a lighter requirement than the direct supervision contrast studies carry.
The NCCI Bundling Trap Most Coders Miss
Here is the rule that causes the most avoidable 70450 denials, and the one most quick guides skip entirely. When a non-contrast head CT (70450) and a contrast head CT (70460) are performed on the same day, in the same session, for the same clinical indication, you do not bill both codes. You bill the combined study code, 70470.
Under National Correct Coding Initiative (NCCI) edits, if 70450 and 70460 are reported together, 70460 is treated as the payable Column 1 code and 70450 becomes the Column 2 code that gets denied. The edit carries a modifier indicator of 1, meaning it can be bypassed only when criteria for a genuinely separate service are met.
The nuance matters. Code 70470 is correct only when the without-then-with study was a single planned protocol from the start. If the contrast scan happened later as a distinct encounter for a new clinical question a different order, a different indication then reporting 70450 and 70460 separately with an appropriate distinct-encounter modifier (such as XE) can be the accurate choice. The documentation has to support which story is true.
Other Modifiers That Apply to 70450
Modifier 76: Repeat Procedure, Same Day
Use modifier 76 when the same provider repeats a non-contrast head CT on the same day for medical necessity for example, to track an evolving bleed. It tells the payer the second scan was intentional, not a duplicate claim.
Modifier 77: Repeat by a Different Provider
When a different provider repeats the scan, modifier 77 applies instead. It serves the same purpose as 76 but signals that the repeat read or study came from someone else.
The X{EPSU} Modifiers Versus 59
When you need to show that 70450 was a distinct service from another procedure on the same day, the specific X modifiers XE (separate encounter), XS (separate structure), XP (separate practitioner), XU (unusual non-overlapping service) are preferred over the broad modifier 59. They tell the payer exactly why the services were separate, which holds up far better under review.
Reimbursement and Documentation Essentials
How 70450 Pays
There is no single flat price. Medicare builds payment from relative value units (RVUs) for physician work, practice expense, and malpractice, then adjusts each by the local Geographic Practice Cost Index and multiplies by the annual conversion factor. Because the code splits into technical and professional components, the site of service shifts the math: physician payment is usually lower in a facility setting, where the facility bills the technical side separately. Commercial payers commonly reimburse somewhere in the range of 120 to 200 percent of the Medicare rate. Always price against the current Medicare Physician Fee Schedule rather than a fixed figure, since the conversion factor and RVUs change every year.
Documentation That Survives an Audit
Clean payment depends on a record that defends the study. At minimum it should include the physician order specifying a head CT without contrast, the clinical indication and symptoms with matching ICD-10 codes, explicit confirmation that no contrast was used, who performed and who interpreted the scan, and the findings. Repeatedly billing 70450 without strong clinical justification is a known audit red flag, so the indication has to be visible on every claim.
Prior Authorization and Coverage
Check the relevant Local Coverage Determination before billing head and neck CT imaging falls under LCD L37373, which lists covered diagnoses. Emergent scans rarely need prior authorization, but elective and repeat imaging often do, and many commercial plans apply their own rules. Verify the payer policy rather than assuming. For practices weighing whether to manage this in-house, our overview of the top medical billing companies walks through what to look for in a billing partner.
Common Reasons 70450 Claims Get Denied
Most denials on this code trace back to a short, predictable list:
- Billing 70450 when contrast was actually used that should be 70460.
- Reporting 70450 and 70460 together instead of the combined code 70470.
- Missing or mismatched ICD-10 codes that fail to justify medical necessity.
- No documentation confirming that contrast was withheld.
- Repeat scans submitted without modifier 76 or 77.
- Ignoring prior-authorization requirements on elective or repeat imaging.
Conclusion
CPT code 70450 earns its place as the fast first read for head trauma, suspected bleeds, and stroke. The code itself is simple; the denials almost never come from the scan and almost always come from the contrast distinction and the 70470 bundling rule. Get those two things right, document why contrast was withheld, and most 70450 claims pay cleanly on the first pass.
If imaging denials are draining revenue your practice has already earned, it pays to work with coders who handle these edits daily. Nexus io radiology billing services pair AAPC-certified radiology coders with payer-specific claim edits to keep studies like the non-contrast head CT moving from order to payment.
Frequently Asked Questions
What is the difference between CPT 70450 and 70460?
70450 is a head CT performed without contrast; 70460 is the same study performed with contrast. The contrast status is the only thing that separates them.
Can I bill 70450 and 70460 on the same day?
Usually not. A same-session without-then-with study is reported as the combined code 70470. Only when the contrast scan is a genuinely separate later encounter can the two be billed separately, and then a distinct-encounter modifier such as XE is needed.
Does 70450 include CT angiography of the head?
No. CT angiography of the head is reported with 70496, a separate code. A non-contrast CT and a CTA are different studies even when ordered together.
When do I use modifier 26 versus TC with 70450?
Use modifier 26 when billing only the interpretation, TC when billing only the scan itself, and no component modifier when one entity provides the complete global service.
Does Medicare require prior authorization for 70450?
Emergent use often does not, but elective and repeat imaging may, and many commercial plans have their own requirements. Confirm the specific payer policy before the scan when possible.