In 2025, prior authorization denials accounted for nearly 11% of all initial claim denials across commercial payers, and denial code 197 sits at the center of that problem. Before discussing how to fix this problem, you first must understand one important distinction between a denial and a rejection.
A rejection is when a claim is stopped at the clearinghouse, and the payer has not seen the claim. A denial means the payer has processed the claim through adjudication, and the payer has decided to deny payment. This distinction will affect how you proceed to resolve either denial type and affect your time for filing an appeal.
This guide breaks down the CO 197 denial code description, its root causes, and the exact steps your team needs to take to resolve and prevent it.
What is Denial Code 197?
Denial code 197 is a standardized Claim Adjustment Reason Code (CARC) maintained by the Washington Publishing Company (WPC), the official body managing HIPAA-mandated code sets used in U.S. claims processing. Its official description reads: “Precertification/authorization/notification/pre-treatment absent.”
Payers post this code on the EOB or the EDI 835 Electronic Remittance Advice (ERA). It means the payer’s adjudication engine found no approved authorization record tied to the submitted CPT or HCPCS code, date of service, and patient benefit plan. In plain terms, the claim was denied because the required prior authorization was either never obtained, not submitted with the claim, or could not be matched to the patient’s active coverage.
Denial code 197 comes almost always with an accompanying RARC. Always check both before taking any action:
- CARC 197 + N210: A missing or invalid prior authorization number. In Medicare DME claims, N210 instructs the biller to append a 14-character Unique Transaction Number (UTN) before resubmission.
- CARC 197 + N706: The submitted procedure requires prior authorization under this patient’s specific benefit plan.
What Does CO 197 Denial Code Mean in Medical Billing?
The CO-197 denial code combines two components, the Claim Adjustment Group Code and the CARC number, each with specific financial weight.
“CO” is for contractual obligation; thus, the provider has the financial responsibility under the payer’s contract. A provider cannot balance-bill a patient for a CO denial; hence, it is up to the practice to “write off” that expense (unless there is an overturn of the denial).
“197” relates to a pre-authorization being required to bill the patient, and therefore, no valid pre-authorization was found during the claim scrubbing process by the payer.
It is also important to recognize the variant codes that may appear alongside or instead of CO 197:
- PR-197 (Patient Responsibility): The financial liability shifts to the patient most often when the patient’s benefit plan requires the member, not the provider, to secure authorization.
- OA-197 (Other Adjustment): Applied in coordination-of-benefits (COB) scenarios or when neither CO nor PR applies cleanly.
In practical billing terms, the co 197 denial code description tells the biller that no pre-service approval was granted and that reimbursement will be withheld until the issue is resolved through corrected resubmission, retroactive authorization, or a formal appeal.
What is Pre-authorization in Medical Billing?
Pre-authorization, also called prior authorization, precertification, or pre-approval, is the formal process of obtaining advance written approval from a patient’s insurer before offering a specific service. Payers use it to confirm medical necessity, manage utilization costs, and ensure treatments align with the patient’s active benefit plan.
Three distinct requirements fall under the CO 197 denial code umbrella:
Pre-authorization/Precertification:
This is the formal approval process initiated by the insurer prior to any services being rendered. The payer will review clinical documentation (i.e., physician notes, nursing notes, etc.) and provide an authorization number for the procedure with an authorized time frame.
Pre-notification:
This allows the insurer to provide advance notice that a service will be provided (typically required for emergency admissions of inpatient hospital services within 24 to 48 hours). No formal pre-authorization will be provided, but if the request is not submitted prior to the service being performed, a CO 197 denial will be processed.
Pre-treatment:
It is predominantly used for behavioral health or dental claims. This is a time when a treatment plan is coordinated and reviewed to ensure that the patient meets the criteria for receiving a service before the treatment plan begins.
Claims form mapping:
It is important for claims submissions. For example, for CMS 1500 (professional claims), the authorization number should be placed in Box 23 or Loop 2300 on an EDI 837P. For UB-04 (institutional/hospital claims), the authorization number should be placed in Form Locator 63 or Loop 2300 on an EDI 837I. Placing the authorization number in the wrong location is a common 197 denial reason, even when there is a valid authorization present.
Medicare Advantage (Part C) note:
Traditional Medicare has limited prior authorization requirements. Medicare Advantage plans operate under private contracts and frequently require authorization for services that traditional Medicare covers without it. Always verify MA authorization requirements separately, never apply traditional Medicare rules to an MA plan.
How to Obtain Pre-authorization?
Verify requirements at scheduling — not at billing:
Before scheduling an appointment for pre-authorization, determine if a CPT/HCPCS code requires pre-authorization by reviewing your insurance’s member portal (or the payer’s website) for all the necessary codes, procedures, and requirements specific to this patient’s health plan and location; there should be a page indicating if there is a pre-authorization requirement.
Gather clinical documentation:
Gather the appropriate clinical documentation (physician orders, relevant diagnostics, letter of medical necessity) and align the language of the documentation to the payer’s clinical criteria sets (MCG or InterQual) to the extent possible.
Submit and log the request:
Once all clinical data is gathered, submit the request as per the criteria specified by the payer. Log the request by entering the date/time of the submission, mode of submission (portal, fax, or EDI), and obtaining a confirmation number. Enter the confirmation number into the accounting records.
Document every detail of the approval:
Document all details pertaining to the auth, such as authorization number, approved CPT codes, and valid period/quantity. If you are submitting a claim, enter the authorization number in the applicable claims field; establish automated follow-ups to remind you to check on the authorization 14 days before it expires.
Confirm authorization before every encounter:
Verify that the authorization is still active immediately prior to each encounter with the patient. If there is a change to the scope of a procedure during an encounter, you must contact the payer within 24 hours to update the authorized CPT code or you will be subject to a new CO 197 denial code for that line item.
Common Reasons for Denial Code 197
No Authorization Was Ever Requested
The team was operating under the assumption that the service was ineligible for the authorization or that the requirement was overlooked during scheduling. In the absence of a pre-authorization on record, the payers’ claim scrubbing engine automatically denies the claim.
Expired Authorization
An authorization for a service has been obtained. However, the service was provided outside of the approved service dates. The most common timeframe for an authorization is 90 days. An example would be an MRI that was authorized to be done on/before March 15 and later rescheduled to March 28; therefore, the claim is denied as CO-197, regardless of the fact that the authorization was obtained for service.
Authorization Scope Mismatch
The billed CPT code does not match the CPT code that was originally authorized for the patient. Payers will match claims to authorizations using exact CPT codes; therefore, if the modifier changed on the procedure that was provided to the patient or if an upgrade occurred on the procedure compared to the original CPT code approved in the authorization, this would break the match and lead to a denial.
Authorization Number Missing from the Claim
An authorization number was obtained but never entered into the appropriate field on the CMS-1500, UB-04, or electronic billing form (EDI 837); thus, the payer has no way to appropriately match the claim to the authorization.
Late Notification for Emergency Admissions
In the case of an emergency admission, the provider must notify the payer of the admission after the fact by submitting a late notification claim within 24-48 hours after the date of admission. Failure to submit this claim in a timely manner will result in a denial of the claim (CO-197) regardless of whether the emergency service was covered.
Undetected Payer Policy Changes
Payers periodically expand authorization requirement lists. A CPT code exempt last quarter may now require auth. Practices that do not audit payer policy bulletins regularly are frequently caught off guard.
How to Manage and Resolve Denial Code 197 (Step-by-Step)
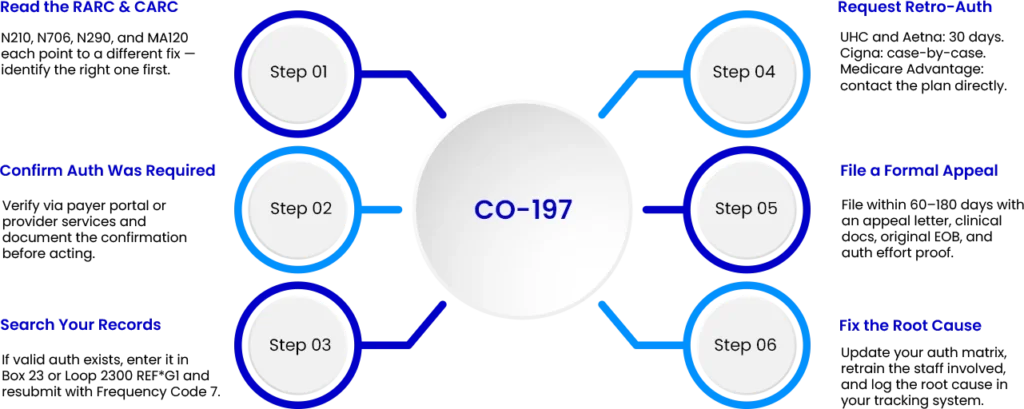
Step 1: Read the RARC alongside the CARC
Pull the EDI835 or EOB for both codes N210, N706, N290, and MA120, which will reference a different CO 197 denial code solution. Do not proceed until you are absolutely sure of what issue the remark code is referencing.
Step 2: Confirm whether authorization was truly required
You will either need to verify through your payer portal or through provider services. Some CO-197 denials are due to payer-system errors. If the payer confirmed that authorization wasn’t required, document the finding in your records and initiate the appeal based on the payer’s confirmation.
Step 3: Search your records
Check your prior authorization log, EHR, and the payer portal’s authorization history. If a valid auth exists covering the date of service and the billed CPT code, you have an administrative error — correct the claim and resubmit using Claim Frequency Code 7 on the EDI 837.
Step 4: Request retroactive authorization
If no auth was obtained, contact the prior authorization department of the payer. UnitedHealthcare and Aetna will accept retro-auth requests for an admin error or if there is clinical urgency, within 30 days of the date of service. Cigna retro-auth cases are reviewed on an individual case basis, so they do allow waivers for the notification of an emergency admission within 48 hours. The Medicare Advantage retro-auth policy varies depending on the plan. Always contact that plan directly.
Step 5: File a formal appeal
If the retro-auth is denied, a formal appeal must be filed within the payer’s timely filing window, which is usually between 60 and 180 days from the date of denial. The appeal letter must include the following:
A formal letter of appeal, which cites medical necessity, complete clinical documentation, physician orders, a copy of the original EOB, and any proof of a good faith effort to obtain an authorization.
Step 6: Fix the root cause
To fix the root cause of CO-197 denials, update your self-created prior auth matrix for that particular payer and provide retraining to the staff member involved in the denial, and log the denial in your tracking system after addressing the CO-197.
Pro-Tip: Build an “authorization scrub” into your pre-submission workflow. Before any claim is submitted, run it against your authorization log. Unmatched claims get held and flagged — not submitted. This single step eliminates the most common cause of CO-197: valid authorizations that never make it onto the claim form.
Conclusion
To summarize, CO-197 denials are preventable, correctable, and resolvable. Your staff needs to be able to differentiate between a CO-197 denial and a rejection. It is important that they review the accompanying remark codes before they can implement a documented resolution workflow. With 33 million people in the Medicare Advantage program by 2026, and an increase in the number of authorization requests by payers, 197 denial reasons will continue to increase for practices that do not have a systematic process for checking pre-authorization prior to submitting claims.
The CO-197 denial reason reflects one common problem of failure to obtain the necessary pre-authorization: missing, expired, mismatched, or improperly entered on the claim. Fix your workflow, and you fix the denial rate. If your team cannot afford to manually track the authorization process, monitor payer policy changes, or appeal denials, exploring a medical billing services partner that handles pre-authorization management and denial resolution as part of a complete revenue cycle workflow is worth considering — particularly if CO-197 denials are recurring across multiple payers or specialties.
To learn more about how Nexus io approaches systematic denial management services, get in touch with our denial specialists today.
